
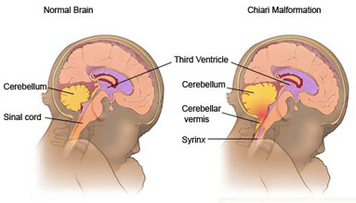
I have added this example picture for you. You can see that the Chiari is found where the Cerebellar Vermis arrow is pointing.
Her skull is a little smaller there than what it should be in that area, so it creates pressure on the Cerebellum, therefore it presses downward.
What are Chiari malformations?
Chiari malformations (CMs) are structural defects in the cerebellum, the part of the brain that controls balance. Normally the cerebellum and parts of the brain stem sit in an indented space at the lower rear of the skull, above the foramen magnum (a funnel-like opening to the spinal canal). When part of the cerebellum is located below the foramen magnum, it is called a Chiari malformation.
CMs may develop when the bony space is smaller than normal, causing the cerebellum and brain stem to be pushed downward into the foramen magnum and into the upper spinal canal. The resulting pressure on the cerebellum and brain stem may affect functions controlled by these areas and block the flow of cerebrospinal fluid (CSF) — the clear liquid that surrounds and cushions the brain and spinal cord — to and from the brain
What causes these malformations?
CM has several different causes. It can be caused by structural defects in the brain and spinal cord that occur during fetal development. This is called primary or congenital CM. It can also be caused later in life if spinal fluid is drained excessively from the lumbar or thoracic areas of the spine either due to injury, exposure to harmful substances, or infection. This is called acquired or secondary CM. Primary CM is much more common than secondary CM.
How are they classified?
CMs are classified by the severity of the disorder and the parts of the brain that protrude into the spinal canal.
Type I involves the extension of the cerebellar tonsils (the lower part of the cerebellum) into the foramen magnum, without involving the brain stem. Normally, only the spinal cord passes through this opening. Type I — which may not cause symptoms — is the most common form of CM and is usually first noticed in adolescence or adulthood, often by accident during an examination for another condition. Type I is the only type of CM that can be acquired. This is the least severe, of the four.
Type II, also called classic CM, involves the extension of both cerebellar and brain stem tissue into the foramen magnum. Also, the cerebellar vermis (the nerve tissue that connects the two halves of the cerebellum) may be only partially complete or absent. Type II is usually accompanied by a myelomeningocele — a form of spina bifida that occurs when the spinal canal and backbone do not close before birth, causing the spinal cord and its protective membrane to protrude through a sac-like opening in the back. A myelomeningocele usually results in partial or complete paralysis of the area below the spinal opening. The term Arnold-Chiari malformation (named after two pioneering researchers) is specific to Type II malformations.
Type III is the most serious form of CM. The cerebellum and brain stem protrude, or herniate, through the foramen magnum and into the spinal cord. Part of the brain’s fourth ventricle, a cavity that connects the upper parts of the brain and circulates CSF, may also protrude through the hole and into the spinal cord. In rare instances, the herniated cerebellar tissue can cause an occipital encephalocele, a pouch-like structure that protrudes out of the back of the head or the neck and contains brain matter. The covering of the brain or spinal cord can also protrude through an abnormal opening in the back or skull. Type III causes severe neurological defects.
Type IV involves an incomplete or underdeveloped cerebellum — a condition known as cerebellar hypoplasia. In this rare form of CM, the cerebellar tonsils are located further down the spinal canal, parts of the cerebellum are missing, and portions of the skull and spinal cord may be visible.
Another form of the disorder, under debate by some scientists, is Type 0, in which there is no protrusion of the cerebellum through the foramen magnum but headache and other symptoms of CM are present.
How common are Chiari malformations?
In the past, it was estimated that the condition occurs in about one in every 1,000 births. However, the increased use of diagnostic imaging has shown that CM may be much more common. Complicating this estimation is the fact that some children who are born with the condition may not show symptoms until adolescence or adulthood, if at all. CMs occur more often in women than in men and Type II malformations are more prevalent in certain groups, including people of Celtic descent.
How are Chiari malformations diagnosed?
Many people with CMs have no symptoms and their malformations are discovered only during the course of diagnosis or treatment for another disorder. The doctor will perform a physical exam and check the person's memory, cognition, balance (a function controlled by the cerebellum), touch, reflexes, sensation, and motor skills (functions controlled by the spinal cord). The physician may also order one of the following diagnostic tests:
An X-ray uses electromagnetic energy to produce images of bones and certain tissues on film. An X-ray of the head and neck cannot reveal a CM but can identify bone abnormalities that are often associated with CM. This safe and painless procedure can be done in a doctor’s office and takes only a few minutes.
Computed tomography (also called a CT scan) uses X-rays and a computer to produce two-dimensional pictures of bone and vascular irregularities, certain brain tumors and cysts, brain damage from head injury, and other disorders. Scanning takes about 3 to 5 minutes. This painless, noninvasive procedure is done at an imaging center or hospital on an outpatient basis and can identify hydrocephalus and bone abnormalities associated with CM.
Magnetic resonance imaging (MRI) is the imaging procedure most often used to diagnose a CM. Like CT, it is painless and noninvasive and is performed at an imaging center or hospital. MRI uses radio waves and a powerful magnetic field to produce either a detailed three-dimensional picture or a two-dimensional “slice” of body structures, including tissues, organs, bones, and nerves. Depending on the part(s) of the body to be scanned, MRI can take up to an hour to complete.
Her skull is a little smaller there than what it should be in that area, so it creates pressure on the Cerebellum, therefore it presses downward.
What are Chiari malformations?
Chiari malformations (CMs) are structural defects in the cerebellum, the part of the brain that controls balance. Normally the cerebellum and parts of the brain stem sit in an indented space at the lower rear of the skull, above the foramen magnum (a funnel-like opening to the spinal canal). When part of the cerebellum is located below the foramen magnum, it is called a Chiari malformation.
CMs may develop when the bony space is smaller than normal, causing the cerebellum and brain stem to be pushed downward into the foramen magnum and into the upper spinal canal. The resulting pressure on the cerebellum and brain stem may affect functions controlled by these areas and block the flow of cerebrospinal fluid (CSF) — the clear liquid that surrounds and cushions the brain and spinal cord — to and from the brain
What causes these malformations?
CM has several different causes. It can be caused by structural defects in the brain and spinal cord that occur during fetal development. This is called primary or congenital CM. It can also be caused later in life if spinal fluid is drained excessively from the lumbar or thoracic areas of the spine either due to injury, exposure to harmful substances, or infection. This is called acquired or secondary CM. Primary CM is much more common than secondary CM.
How are they classified?
CMs are classified by the severity of the disorder and the parts of the brain that protrude into the spinal canal.
Type I involves the extension of the cerebellar tonsils (the lower part of the cerebellum) into the foramen magnum, without involving the brain stem. Normally, only the spinal cord passes through this opening. Type I — which may not cause symptoms — is the most common form of CM and is usually first noticed in adolescence or adulthood, often by accident during an examination for another condition. Type I is the only type of CM that can be acquired. This is the least severe, of the four.
Type II, also called classic CM, involves the extension of both cerebellar and brain stem tissue into the foramen magnum. Also, the cerebellar vermis (the nerve tissue that connects the two halves of the cerebellum) may be only partially complete or absent. Type II is usually accompanied by a myelomeningocele — a form of spina bifida that occurs when the spinal canal and backbone do not close before birth, causing the spinal cord and its protective membrane to protrude through a sac-like opening in the back. A myelomeningocele usually results in partial or complete paralysis of the area below the spinal opening. The term Arnold-Chiari malformation (named after two pioneering researchers) is specific to Type II malformations.
Type III is the most serious form of CM. The cerebellum and brain stem protrude, or herniate, through the foramen magnum and into the spinal cord. Part of the brain’s fourth ventricle, a cavity that connects the upper parts of the brain and circulates CSF, may also protrude through the hole and into the spinal cord. In rare instances, the herniated cerebellar tissue can cause an occipital encephalocele, a pouch-like structure that protrudes out of the back of the head or the neck and contains brain matter. The covering of the brain or spinal cord can also protrude through an abnormal opening in the back or skull. Type III causes severe neurological defects.
Type IV involves an incomplete or underdeveloped cerebellum — a condition known as cerebellar hypoplasia. In this rare form of CM, the cerebellar tonsils are located further down the spinal canal, parts of the cerebellum are missing, and portions of the skull and spinal cord may be visible.
Another form of the disorder, under debate by some scientists, is Type 0, in which there is no protrusion of the cerebellum through the foramen magnum but headache and other symptoms of CM are present.
How common are Chiari malformations?
In the past, it was estimated that the condition occurs in about one in every 1,000 births. However, the increased use of diagnostic imaging has shown that CM may be much more common. Complicating this estimation is the fact that some children who are born with the condition may not show symptoms until adolescence or adulthood, if at all. CMs occur more often in women than in men and Type II malformations are more prevalent in certain groups, including people of Celtic descent.
How are Chiari malformations diagnosed?
Many people with CMs have no symptoms and their malformations are discovered only during the course of diagnosis or treatment for another disorder. The doctor will perform a physical exam and check the person's memory, cognition, balance (a function controlled by the cerebellum), touch, reflexes, sensation, and motor skills (functions controlled by the spinal cord). The physician may also order one of the following diagnostic tests:
An X-ray uses electromagnetic energy to produce images of bones and certain tissues on film. An X-ray of the head and neck cannot reveal a CM but can identify bone abnormalities that are often associated with CM. This safe and painless procedure can be done in a doctor’s office and takes only a few minutes.
Computed tomography (also called a CT scan) uses X-rays and a computer to produce two-dimensional pictures of bone and vascular irregularities, certain brain tumors and cysts, brain damage from head injury, and other disorders. Scanning takes about 3 to 5 minutes. This painless, noninvasive procedure is done at an imaging center or hospital on an outpatient basis and can identify hydrocephalus and bone abnormalities associated with CM.
Magnetic resonance imaging (MRI) is the imaging procedure most often used to diagnose a CM. Like CT, it is painless and noninvasive and is performed at an imaging center or hospital. MRI uses radio waves and a powerful magnetic field to produce either a detailed three-dimensional picture or a two-dimensional “slice” of body structures, including tissues, organs, bones, and nerves. Depending on the part(s) of the body to be scanned, MRI can take up to an hour to complete.
